
Epidemics
In the previous blog (2.7 Covid–19 part 1) we saw what a virus is and how it gets to destroy cells in the body. We also touched on how the immune system can be stimulated by vaccination to eliminate the virus. In normal circumstances our immune systems are coping continuously with the threats that surround us on a daily basis.
They generally succeed – that’s how we stay healthy. Since birth we have been building up a wonderful repertoire of different antibody molecules to fend off microbes. Our vaccinations help this process wherever possible.
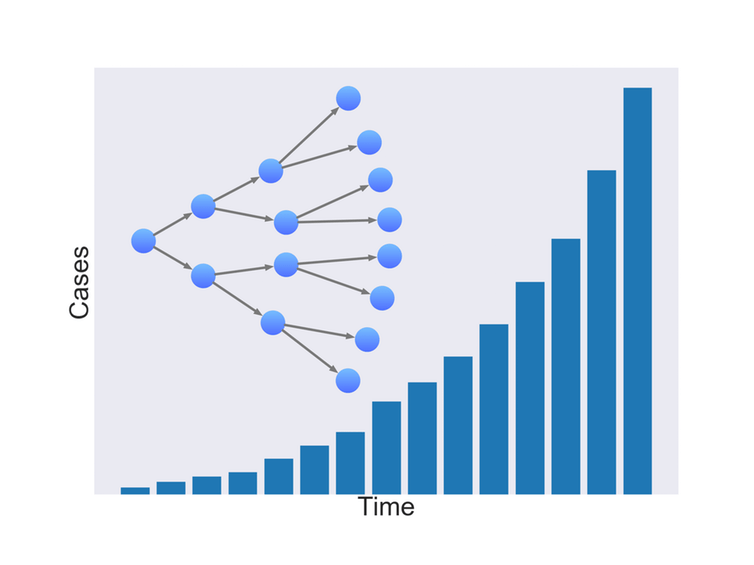
But, as we all know only too well, this doesn’t always work. We still get colds and flu. Bugs can be “passed around” but eventually they die out. A bout of colds arises when, on average, one person infects more than one other person: the bug spreads.
They die out when an infected person infects less than one other, on average over a given population. As this graph exemplifies in the case of flu, numbers rise gently at first, then steeply, then peak or flatten off and ultimately die away in reverse fashion.
Serious epidemics occur when the infectious agent passes easily and rapidly from person to person. The degree of seriousness depends on many factors including the length of the incubation period, the virulence of the bug, the geography of the population and its social behaviour.
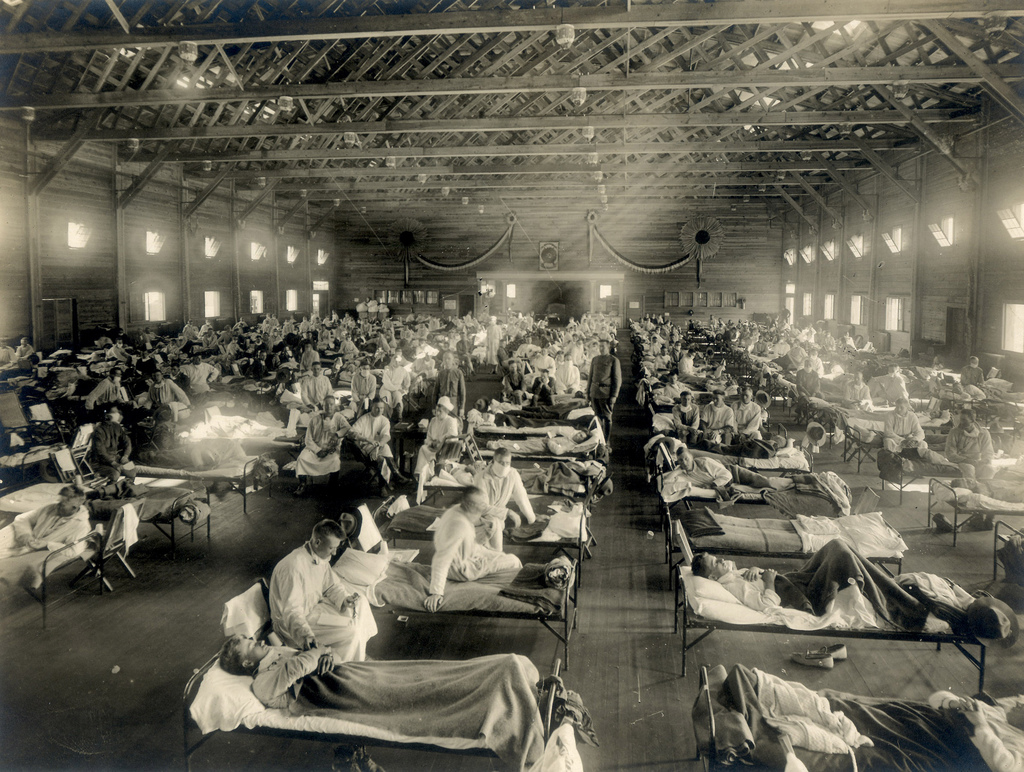
This photo of an emergency hospital in Kansas during the 1918 influenza epidemic (courtesy of wikimedia) reminds us that epidemics are not just a creature of globalisation but have occurred throughout history – from Athens (430 B.C.) via the Black Death (1340s/50s) to HIV, Ebola and Zika in more recent times.
For the COVD-19 epidemic an infected person is thought (as of 22nd March) to pass the virus on to between 2 and 2.5 other people on average[i]. For seasonal flu, the figure is around 1.5.
Symptoms were first noted in December 2019 in Wuhan[ii]. It is believed the virus may have originated in bats. It spreads via droplets produced during coughing, sneezing and normal breathing out and may also spread from touching contaminated surfaces and then touching your nose, mouth or eyes. It is most contagious when people actually exhibit symptoms, although spread is also possible before this. It takes from two to fourteen days, five on average, to develop symptoms after infection.
Young people seem to be less affected with those under 20 accounting for 2.4% of cases worldwide, as of 26th February. Around 80% of deaths were in those over 60, of whom 75% had pre-existing health conditions.
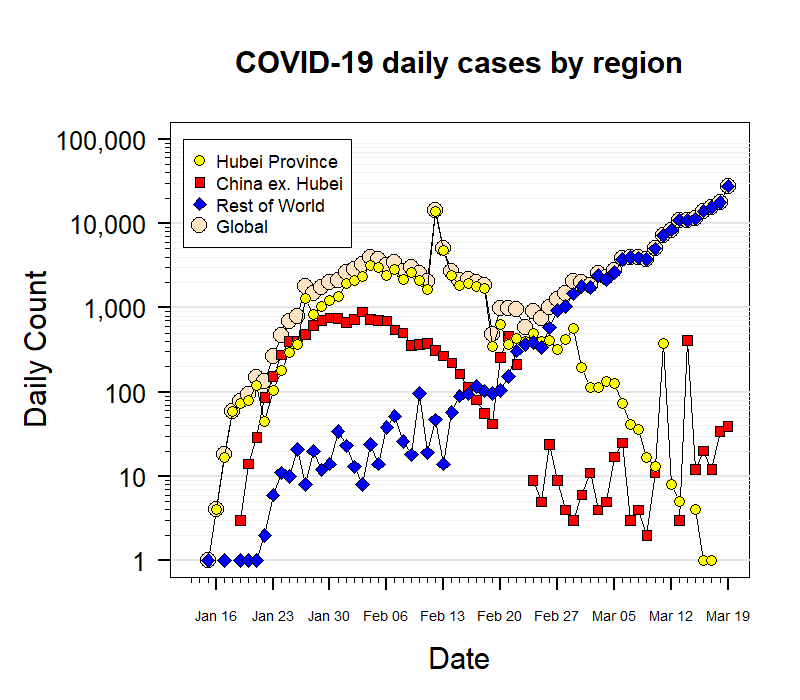
Data from around the world is being used to track the effects of different responses. The graphs below show how, on the date of writing, 19th March 2020, it peaked and fell dramatically in Wuhan province. In China generally it peaked but has not fallen to such a low value as Wuhan. All this is liable to change over the coming days and weeks. In the rest of the world it is climbing exponentially. The vertical scale is logarithmic which means that the straight-ish part of the blue line shows the growth is exponential – you can see it rises from 100 to 1,000 to 10,000 in roughly equal periods of time.
Protecting yourself
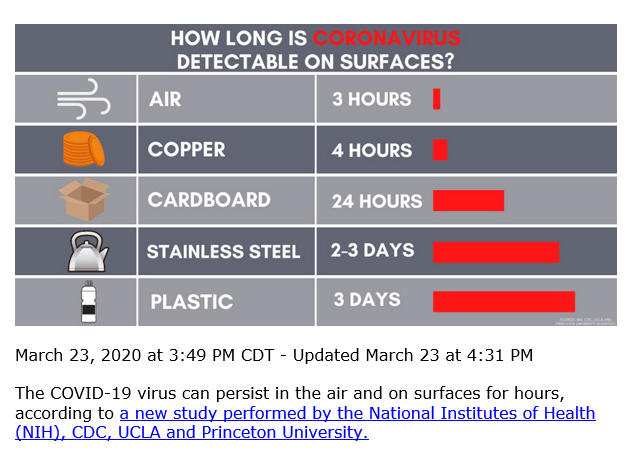
The virus is believed to last on surfaces for about the same time as previous corona viruses. One study shows that from droplets in air it is able to infect people for at least three hours, on plastic up to three days, on cardboard one day and on copper up to four hours. They hadn’t yet tested other surfaces like wood or glass or textiles.
These apparently clear cut figures from laboratory study need a bit of interpretation as we apply them to our daily lives. First the amount of virus falls off exponentially, which means it halves in a given period (half-life), then what’s left halves in the same period and so on. So, for example,
in a droplet in air it takes about 66 minutes for half the virus particles to become inactive, so after 132 minutes three quarters will be inactivate but 25% will still be viable.
On stainless steel, the half-life is 5 hours 38 minutes
On plastic, it’s 6 hours 49 minutes
On cardboard, it’s about 3 hours 30 minutes hours,
So, although it appears the virus never completely disappears, I guess the less there is, the less you might pick up and the more effective your body’s defences will be in fighting it off (I’d be grateful to hear if anyone has better information about this) .
A Princeton scientist on a recent BBC radio programme also pointed out that the virus may cling on to surfaces such as cardboard more strongly, so be less easily transferred by touch. The upshot of this early research is that we should be cautious about surfaces, disinfecting them regularly.
You can disinfect contaminated surfaces with alcohol-based liquids (with 62–71% ethanol or 50–100% isopropanol) or bleaching agents (with 0.1% sodium hypochlorite or 0.5% hydrogen peroxide). You can check the ingredients on the label; my regular spray-on bleach solution contains one of these. Outside the human body, the virus is vulnerable to soap and alcohol. Surgical masks are recommended for people who may be infected and for those taking care of someone who may have the disease. For healthy people, they are recommended only for those at high risk (e.g. caring for an infected person).
The Government website[iii] summarises its advice for households as follows:
Cleaning: usual household products, like detergents and bleach are OK for frequently touched surfaces such as door handles, handrails, remote controls and table tops.
Hydration: drink enough water to keep your urine a pale clear colour.
Medications: Over-the-counter medicines such as paracetamol are fine
Facemasks: are only recommended for clinical settings
Social visitors: should not enter your home
Animals/pets: there’s no evidence that they can be infected
Protecting the population
In the early stages of an outbreak, containment is required – tracing and isolating infected people. In the next stage – mitigation – measures are taken to slow the spread and mitigate its effects on the health care system and society. A third stage – suppression – requires more extreme measures in order to reach the point where each case of infection only goes on to infect less than one other, on average – this is the stage we now are in. The positive news as of 30th March, from the Imperial College team monitoring the process, is
“We cannot say for certain that the current measures have controlled the epidemic in Europe; however, if current trends continue, there is reason for optimism” [iv]
But restrictions will need to continue for a long time to avoid a new upsurge (see Read More below).
A recent BBC programme pointed out that the highly contagious nature of the Covid-19 virus (SARS-Cov-2), compared to its cousin SARS 1, may not be due so much to its duration on surfaces but to the long incubation period during which a person experiences no symptoms. It has recently become clear from a complete survey of a town in China that 4 out of 5 transmissions were from people without symptoms. Similarly, in the town of Vo in Italy, a survey of all residents showed that only a quarter of people who carried the virus actually had symptoms. Some incorrect information was circulated earlier, suggesting people without symptoms could not infect others.
In China, once the severity of the outbreak became apparent, entire cities were quarantined. In South Korea the largest and best-organised program in the world involved screening the population (included drive-thru testing with next-day results), and isolating any infected people as well as tracing and quarantining those who contacted them. It is considered to be a success in controlling the outbreak despite not quarantining entire cities. Singapore provided financial support for those infected and imposed large fines for those who failed to quarantine themselves.
The World Health Organisation (WHO) has urged countries to “test, test , test”. Testing for the presence of the virus is done be using respiratory or blood samples from which the RNA (similar to DNA) of the virus can be detected. RNA is the genetic material of the virus and is a unique identifier for each type – COVID 19, for example. Results are generally available within a few hours to days. A different test checks retrospectively whether someone has had the disease and become immune, by testing for the presence of antibodies. These are produced naturally by the immune system in anybody who has had the virus. This type of test is important as some people will become immune without having realised they had had the disease – it can be so mild in some cases.
With most known infections, once you have had it, you become immune, at least for a while. In the case of COVID-19, evidence on this is not yet available. The UK government’s chief scientific adviser Sir Patrick Vallance and chief medical adviser Prof Chris Whitty, say “those who have had the virus once will develop some immunity – and it is rare to get an infectious disease again”[v].
You can read about “herd immunity” in the Read More section below.
Social behaviour.
It’s pretty clear from recent statements from leaders in both science and government that the short term future of the epidemic depends critically on whether people change their everyday behaviour in simple but important ways. Unknown to most of us, scientists (including social and economic ones), are carrying out experimental and survey research continuously on this.
The messages about hand washing, keeping a distance from others and using public transport are not just dreamed up because they sound sensible. They have been rigorously tested.
Take the example of hand washing[vi]. Research shows that washing with water alone reduces germs by 50% – but adding soap reduces them by 80%[vii]. Yet people report that they wash their hands much more often than they actually do, and they wash less when they think they are not being observed.
A summary of research evidence suggests the following barriers and strategies for changing behaviour:
lack of awareness: people may simply not realise how well specific handwashing actions can prevent the spread of infectious disease.
drawing attention being drawn to something less effective: People are more likely to see wearing masks as visible and novel, unlike washing of hands.
risk “thermostat”: if you protect yourself in one way you may feel freer to take risks in another.
availability of water, soap, and drying materials. simply increasing this helps improve hand hygiene: dispensers need to be well located (e.g. by a lift) and brightly coloured
People can be particularly prone to biased decision-making in an epidemic which may make them less willing to take up preventive behaviours[viii] because:
Outcomes are uncertain. you have no way of knowing if taking preventive steps will actually stop them contracting the virus. You’ll never know what didn’t happen.
Many of the benefits of containment accrue to other people, particularly if the person taking preventive steps is already infected.
The potential benefits of not getting ill are in the future, but the effort of taking preventive steps is felt in the present (e.g. changing hand-washing habits)
Here are some principles for government communications based on behavioural research:
- Maintain public trust: doctors and scientists are the two most trusted professions in Britain. Politicians and government ministers are among the least [ix].
- Make messages clear, simple and precise. When people are concerned about a threat, they process information less effectively. Less information may lead to more accurate judgements. Clear, easy to remember instructions are more likely to be followed.
- Be transparent: showing what the authorities are doing behind the scenes to help people and deal with the situation may improve perceptions of those actions[x]. Social media is a good vehicle for this.
Social behaviour on the larger scale clearly depends on the extent to which individuals decide to follow guidance provided by authorities. Extracts from two sources of research on this are in the Read More section below. One outlines the types of people most likely not to comply: refusers, deniers, the young, religious/cultural outliers. The other identifies six principles of influence that generate compliance: reciprocation, commitment/ consistency, authority, social proof, scarcity, liking.
That’s enough on epidemics and how we respond to them. Next I‘d like to think about how the general public cope with relevant mathematical concepts – risk, chance, quantity, exponential spread, peaks and gradients etc …. Let me know if you have any thoughts or queries.
© Andrew Morris 29th March 2020
ii https://www.livescience.com/first-case-coronavirus-found.html
vii https://www.ncbi.nlm.nih.gov/pubmed/21318017
viii https://www.bi.team/blogs/covid-19-how-do-we-encourage-the-right-behaviours-during-an-epidemic/
ix https://www.ipsos.com/ipsos-mori/en-uk/its-fact-scientists-are-most-trusted-people-world https://www.hbs.edu/faculty/Publication%20Files/14-115_aee7737a-a405-46f1-85e9-67882dd95435.pdf
x https://www.hbs.edu/faculty/Publication%20Files/14-115_aee7737a-a405-46f1-85e9-67882dd95435.pdf
xi https://medium.com/wintoncentre/how-much-normal-risk-does-covid-represent-4539118e1196
xiii https://www.imperial.ac.uk/news/196234/covid19-imperial-researchers-model-likely-impact/
