
The Ebola vaccine took five years to develop. Penicillin was discovered by accident. Developing effective drugs and vaccines is laborious, time consuming and chancy. But there’s plenty of room for hope in present circumstances. Back in the 1970s, when I was working on a drug for asthma, the game was known colloquially as “molecular roulette”. You’d have a guess at a suitable molecule, make hundreds or even thousands of variations of it and try each one out on yeast or insects or mice. Maybe one or two might have a positive effect, maybe not.
In the case of sodium cromoglycate, the molecule I worked with, the guess had been based on a plant grown in the Middle East known to relax muscles. The guess was that something in the plant might relax the airways of asthmatic patients. After much purification and isolation, a substance was found that was active against asthma. The original researcher, a sufferer from the condition himself, tried it out on himself. Later, its mechanism of action was found to have nothing to do with relaxing muscles; instead it inhibited certain chemicals known to be involved in the allergic response. Guesswork had inspired the investigation but chance had determined the outcome.
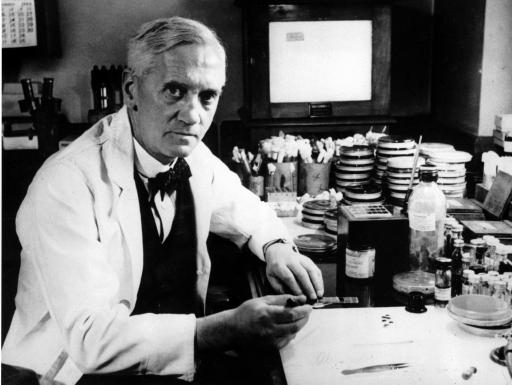
The effect of penicillin was originally noticed by Alexander Fleming, who had left a petri dish of staphylococcus bacteria growing in his lab, while he went on holiday. On his return he found a fungus had grown on part of the dish which appeared to have killed the surrounding bacteria. Miraculously, he didn’t throw away the mouldy dish but chose to pursue his curiosity instead. After further purification and refinement he isolated the active ingredient and named it penicillin, after the name of the fungus.
Alexander Fleming with petri dishes
Fleming found it hard to produce at scale, however, and believed it would not last long in the body. He had made the discovery but not been able to develop a viable, mass-produced drug. In a fine example of the downstream complexity of developing a practical drug, work on this was picked up elsewhere, by other scientists at the Radcliffe Infirmary in Oxford – Ernst Chain and Howard Florey.
Scientists today are making it clear to the public that developing drugs to treat Covid-19 or a vaccine to protect against it will take some time. In addition there is no certainty that either will prove possible. Before looking into the prospects for vaccines and drugs for the coronavirus, let’s look more closely at how such precious molecules have their effects on the body.
Drugs and receptors
Like most of the chemicals we encounter in biology, drugs and vaccines are molecules – i.e. they’re composed of many atoms bonded together. They are inserted into the body in order to interact with other molecules that are part of the body. Many drugs (though not all) are relatively small molecules which secure their effect by interacting with the mostly larger molecules that make up our bodies. A familiar example is aspirin which interacts with a much larger protein molecule with the catchy name of cyclooxygenase (or COX).
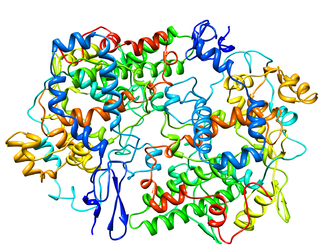
The models show the aspirin molecule (on the left) and the cyclooxygenase receptor molecule (above). They are not to scale: the receptor molecule is reduced in size to fit the page – it’s around 400 times heavier than aspirin. The aspirin model shows all twenty one individual atoms in the molecule; the receptor model simply shows the general direction of the long chain of the molecule comprising thousands of atoms.
In general, drugs interact with molecules that normally carry out some bodily function, like moving a muscle or digesting food. Drugs may either inhibit or block their action or enhance it in some way. The aspirin receptor molecule, for example, is an enzyme that normally helps to dilate blood vessels as part of the body’s inflammatory response when the body is injured in some way. Aspirin inactivates this receptor molecule, quelling the inflammation as a result.
Another well-known example is the beta blocker, a drug which as, it says on the tin, blocks action. In this case it prevents adrenalin from over-stimulating the heart. Statins work in a comparable way, by inhibiting an enzyme molecule: in this case, one is that essential for the production of cholesterol.
So how exactly do small drug molecules inhibit, block or in some cases enhance, the action of a large molecule – often an enzyme? The clue is in the way enzymes work. As explained in blog 2.4 Enzymes in this series, these large molecules, carry out some function at a particular spot on their surface known, for self-explanatory reasons, as the active site. A typical function of many enzymes is to break a bond between two atoms in some other molecule, thus splitting it up; or it may do the opposite: bond together two separate molecules to make a larger one. Enzymes can be thought of, in this regard, as tools. As can be imagined, a drug that inhibits or blocks an enzyme’s normal action simply fits nicely into the space of the active site, preventing the normal action from taking place. It’s like a key that sits in the lock to prevent another key entering.
This image shows how a statin molecule helps cut your cholesterol level.
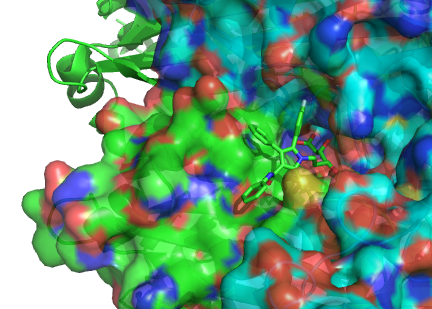
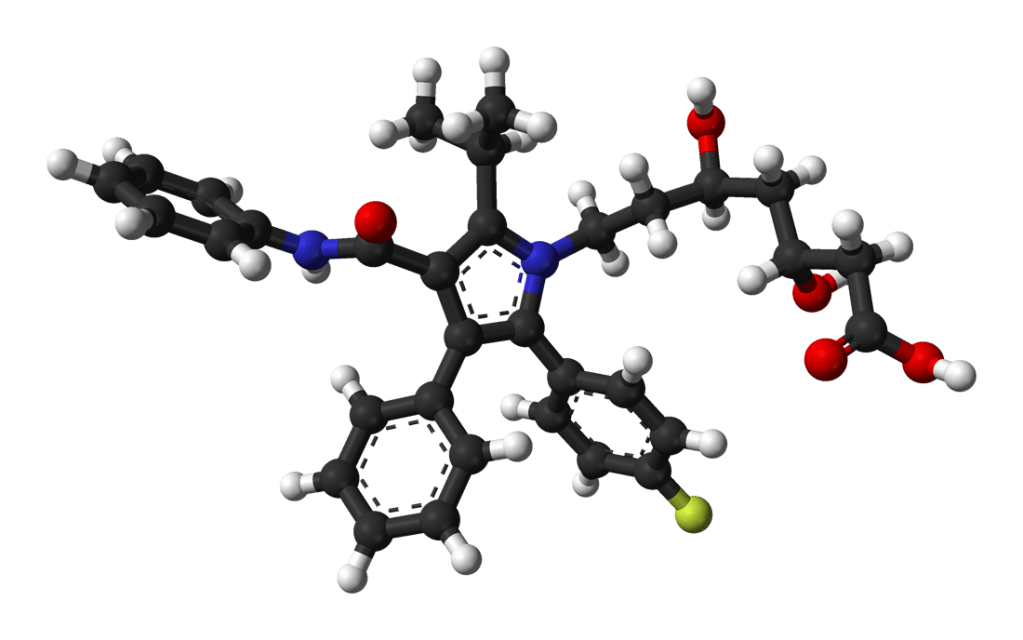
The model on the left represents a statin molecule. In the model above the statin molecule is the light green stick model in the middle. The big blobby thing in red, blue and green is a model of the statin receptor – an enzyme. The bit of its surface where the little statin molecule is sitting is the active site.
In the absence of a statin, a small molecule present in the cell will find its way into this site, thereby activating the enzyme and triggering a chain of events leading to the production of cholesterol in the liver. By getting in the way of this, the statin molecule stops the chain of events, thus helping to reduce the level of cholesterol circulating in the body.
Drug design
Thanks to an array of advances in recent decades the chances of finding effective drugs have increased enormously. Where once pharmacologists and medicinal chemists had to forage in the dark, following up hunches and testing vast numbers of candidate molecules, today drugs are increasingly developed by design. With the aid of X-ray crystallography and other imaging techniques the precise shape of the active sites of receptor molecules can often be surveyed. Candidate drug molecules can then be synthesised or discovered in living things that look as though they might fit the site. As you can imagine, many subtle factors are involved – not only the physical shape of a molecule but the distribution of electrical charge over its surface, for example.
Many other factors will determine whether a candidate molecule is effective or not. Will it pass unscathed through the stomach? Will it make its way into the bloodstream so that it reaches the relevant organs? Will it stay intact long enough? Even more critical: will it prove toxic, will it affect other receptors, producing unwanted side effects? For these reasons many stages of laboratory testing are needed to check that it might be effective and safe.
After the laboratory work, trials are needed on living systems – perhaps microorganisms, plants or animals and ultimately human volunteers. Not only must the safety and effectiveness be checked at each stage, but the means of delivery – pill, inhaler, injection, drip – has to be designed so the drug can administered effectively. Finally, dosages have to be worked out for various types of user – children, adults, pregnant women and so on. Overall, a huge, time consuming and costly process. Ten to fifteen years is considered a reasonable expectation of the time needed[i]. A recent study[ii] put the average cost at around $2.5 billion.
If you have time, an explanation of how vaccines are developed can be found at the end of this blog.
Coronavirus
What is happening in the case of coronavirus? Hundreds of labs across the world are working at extraordinary speed, with greatly expanded resources, to develop a drug to interfere with the progress of the virus in infected people and a vaccine to offer immunity to those not yet infected.
The course of a viral infection has many stages and an assault on it can be mounted in any of many different ways. Military metaphors are generally not a good idea in biology – they tend to create the impression of an enemy that has a plan, an objective, a strategy. The plain truth is that viruses just plough on doing their reproductive thing without any plan or purpose. It’s what they do.But to illustrate how wide is the range of options for interfering with a virus the metaphor helps. Battles are not just about the frontline: munitions, food supplies, communications, reinforcements and many other resources also contribute. A viral attack, similarly, has multiple aspects.
First, the coronavirus has to reach cells in the respiratory system and enter them in order to reproduce itself. The large ‘spike’ protein in its surface docks onto the lung cell for this purpose, so drugs are being investigated that might block this. A drug could perhaps lock onto the spike protein or incapacitate it.
This rather complicated diagram illustrates three ways in which this might happen (each marked with a cross X through a red arrow). The virus with its ’spike’ proteins is on the left, the human cell on the right.
The top two images show the receptor on the cell being blocked by potential drug molecules (in blue). The bottom image shows the virus particle itself being incapacitated by a more complex assembly of molecules (blue and brown).
An alternative strategy would be to design a drug that interferes with the reproductive mechanism of the virus by interfering with its RNA (similar to DNA). This is how the drug Remdesivir, originally developed against the Ebola virus, works. A different approach would be to disable parts of the cell itself that enable the virus to reproduce and burst out to wreak further damage. A completely different approach would be to address the immune system rather than the virus. Some of the worst symptoms are cause by immune overreaction, causing excess debris which clogs up the airways. A drug could potentially dampen this reaction.
A quite distinct set of investigations is also being made in various labs across the world, aimed not at interfering with the virus itself but at reducing the damage caused by the symptoms[i]. Drugs already approved as safe and effective in one context can simply be tested for efficacy against Covid-19. One kind are drugs that dampen the immune system, such as those used in rheumatoid arthritis. These could prevent an immune overreaction from blocking the airways. Another kind, used for treating high blood pressure could prove useful. The molecule of this drug blocks certain receptors that would otherwise provide entry into cells. Perhaps this might act to prevent the virus from entering cells.
Different teams throughout the world are choosing different paths to follow, according to their skills, resources and previous experience. This multiplicity is extremely helpful given the complexity of the drug development process: no-one can predict which approach might prove successful.
Prospects
Thus by manipulating various types of molecule – small inhibitors, larger proteins or stretches of RNA – scientists in hundreds of labs are pursuing individual projects aimed at designing, synthesising and testing a wide range of remedies. As candidate molecules emerge from laboratories around the word, trials will take place at small, medium and large scale, to check whether they are safe, effective and produce lasting effects. If any of them pass these tests, practical issues of mass production and distribution arise. There will presumably be economic questions about setting the price and deciding who should bear the cost. Then there will be extraordinary logistical challenges about manufacturing at such scale and making it available throughout the world. Will there also be moral questions about who is to be first in the queue? Will this prove an opportunity for the world to come together for the greater good or will fortunate companies and countries seek to gain advantage? It’s easy to be pessimistic about these choices, given the weak condition of important international organisations. It’s worth recalling, however, that Tim Berners-Lee chose the ethical route when he made his invention of the world wide web available to the entire world without charge or patent restriction. Science is playing critical part in revealing pathways to ending the pandemic but, as an epidemiologist at the University of Chicago puts it: “how the pandemic plays out is at least 50% social and political”[ii].
Andrew Morris 8th July 2020
Further reading
Vaccines
A vaccine is a rather special case of a molecule deigned to interact with molecules in the body. It is designed to activate a particular system in the body: the antibody system. Antibodies are giant molecules, part of the extensive and complex immune system. These molecules are capable of ‘recognising’ a molecule that is not part of the body and help dispose of it. Antibody molecules have an extraordinarily adaptive structure which enables them to shape their active site to complement any one of thousands of potentially harmful molecules. As an aside, they also recognise unfamiliar molecules on transplanted tissue, which unfortunately leads the body to reject transplants from unrelated donors.
We inherit some types of antibody from our mothers before and after birth, which enables us to fight off some infections as infants. But we also develop new types of antibodies as we progress through life, encountering ever more kinds of bug. Our immune system creates new types of antibody to counter the new types of threatening molecule it comes across. For this reason it is rightly called the ‘adaptive’ immune system.
When we say an antibody molecule ‘recognises’ a new threatening pathogen, it means that it fits its shape around some part of the surface of that pathogen.
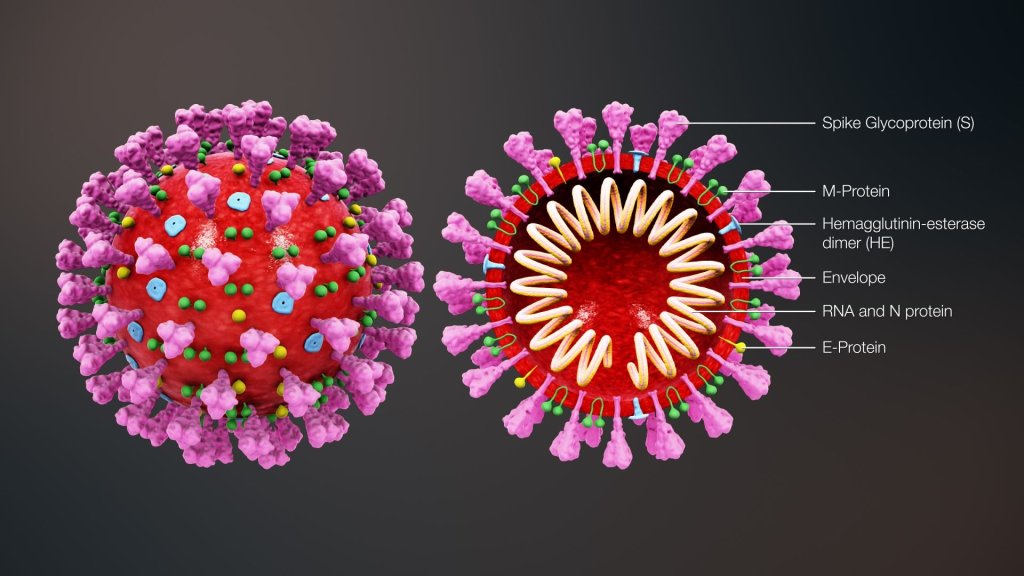
In the case of the coronavirus, as with many other bugs, it is part of a particular protein molecule on the complex surface of the virus particle that is ‘recognised’. As the illustration show, there are three types of protein on the surface of the coronavirus, shown in pink, green and yellow.
It is the pink ‘spike’ glycoprotein (protein with sugar molecule attached) that enables the virus to attach to cells in the respiratory system. Antibodies would need to ‘recognise’ (i.e. fit their structure around) part of this prominent protein on the surface of the virus.
Unfortunately, our immune systems have never encountered this particular version of a coronavirus before so do not have antibodies shaped to fit it, ready to hand. Once a person has been infected, however, the immune system creates a new antibody type specific to this COV-2 SRAS virus which, for those who survive, succeeds in defeating the infection. As we know from the infections we once had as children which never return, our immune system not only fights off microbes but retains a ‘memory’ of them. More accurately it retains a small number of ‘archive’ copies of the specific antibody that defeated them, ready to be multiplied up when needed.
The role of a vaccine is to fool the immune system into creating these specific antibodies and to retain archive copies of them, without actually invoking the disease itself. One way to achieve this is by mimicking the crucial part of the surface protein that the antibody recognises, but not the whole virus. This enables the immune system to produce the right antibodies, precisely shaped to tackle a specific virus and to store archive copies of them. Were the vaccinated person to encounter the virus at some later stage, they would already have the antibodies needed to defeat it. They would be protected or ‘immune’.
Drug developers are working to develop disabled versions of the virus or bits of the spike protein on its surface that can be injected into the body to stimulate production of antibodies that will lie in wait should the virus enter their respiratory system one day.
An alternative strategy involves manipulating the gene rather than the protein part of the virus. The virus’s genetic code, its RNA, was quickly worked out by scientists in China and made freely available to scientist around the world shortly afterwards. This enables vaccine developers to take the gene within the RNA that codes for the ‘spike’ protein, for example, and insert this into the RNA of a different, safe virus. This would be injected into healthy bodies which would, as a result, start manufacturing the spike protein inside their healthy cells. These ‘alien’ spike proteins would then be identified by the immune system which would go on to produce antibodies to them. The person would be protected were the actual coronavirus to infect them subsequently. They would become immune.
[i] Livescience downloaded July 2020 https://www.livescience.com/coronavirus-covid-19-treatments.html
[ii] Scientific American June 2020 p.39.
[i] zmescience article downloaded July 2020. https://www.zmescience.com/other/science-abc/drug-development-trials-pharmacy/
[ii] Scientific American article downloaded in July 2020. https://www.scientificamerican.com/article/cost-to-develop-new-pharmaceutical-drug-now-exceeds-2-5b/#:~:text=A%20new%20report%20published%20by%20the%20Tufts%20Center,over%20the%20estimate%20the%20center%20made%20in%202003.
