
A common problem with the circulatory system, for which we are routinely checked, is high blood pressure. Persistent high pressure, a condition known as hypertension, is generally attributable to narrowing of small arteries and arterioles. There’s a variety of causes for this narrowing, including damage to the lining of the blood vessel walls, inflammation and imbalances in the concentration of the ions sodium and potassium. Explanations differ according to age, genetic inheritance, diet and other environmental and physiological conditions. Countless studies show that hypertension is reduced with a healthy, varied diet, regular exercise, moderation alcohol consumption and absence of smoking.
“What about cholesterol – doesn’t that have something to do with blocked arteries?” asked Sarah in a discussion on the topic. “How does that work – what is it, come to that?” she added.

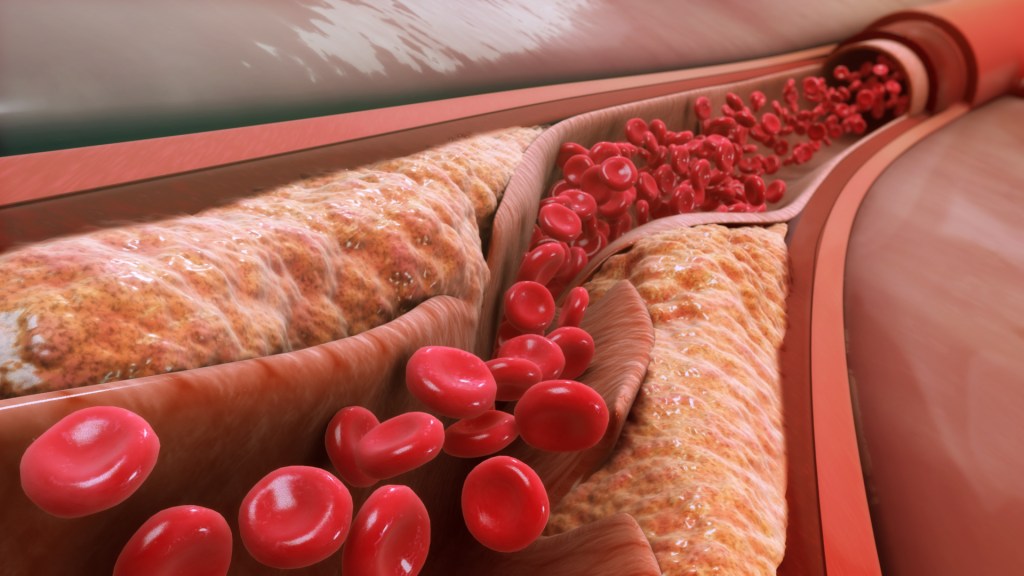
A common cause of narrowing is a thickening of the walls inwards by the growth of so-called plaques. These are places where various types of debris have accumulated (figure 11). The build-up is within the wall, rather than in the interior of the tube itself.
Figure 11 Plaque at the junction of two arteries
The plaque is made up of cholesterol, fatty substances, debris from dead cells, fibrous tissue and other waste. This material causes the wall to swell and, in particular, to push inwards, thus reducing the space within the tube of the blood vessel through which blood flows (figure 12).
Figure 12 plaque causing an artery to narrow (model).
This narrowing, known technically as arteriosclerosis, is the basis of various conditions in the heart and brain caused by poor blood flow. Insufficient supplies of oxygen and vital nutrients carried by the blood means that cells, and therefore tissues, may die. If this occurs in the brain, the result is a stroke. This is often the result of a blood clot, or other particle, jamming in an artery narrowed by plaque. It can lead to restriction in the flow of vital ingredients or to bursting of the blood vessel (haemorrhage). Cells then die off due to lack of oxygen and glucose, vital for the functioning of any cell.
The arteries that supply the heart muscles are also vulnerable to narrowing. By restricting the flow of vital oxygen and nutrients this may damage the cells of the muscle and lead to a range of conditions. An inadequate supply of oxygen may lead to angina, causing discomfort or pain during exertion. More seriously, complete blockage of an artery serving the heart muscle can result in a heart attack (or infarction). This causes muscle cells in the neighbourhood of the blocked artery to die, thus weakening the heart.
Cardiac arrest, on the other hand, is an electrical control fault rather than a failure of power in the muscles. This can occur in several different ways. In the most common, known as ventricular fibrillation, electrical activity becomes uncoordinated, disrupting the regular beat. The most common underlying cause is damage to the heart muscle resulting from narrowing of the arteries. Other causes can be structural problems in the heart tissue, perhaps resulting from high blood pressure over an extended period. These are more common in older people. Genetic mutation is yet another possible cause of cardiac arrest, more common amongst younger people. These can impair the proper movement of electrically charged particles (ions) in the muscle cells, upsetting the rhythm of electrical activity. Other causes, only too familiar from sad reports in newspaper, include drug overdoses, drowning, poisoning and trauma.
Treatments
An amazing array of treatments have been developed to deal with various disorders of the heart. Here we describe just a few. The most fundamental is simply to follow the guidance on healthy living. It’s now well-evidenced and well-publicised: avoid smoking, take exercise and moderate your intake of saturated fats and sugars. These reduce the chances of narrowing the arteries, the cause of so much heart disease.
Sarah had raised the question of cholesterol in a discussion group. “What is it? What should we be doing about it? What do statins do” she had asked.
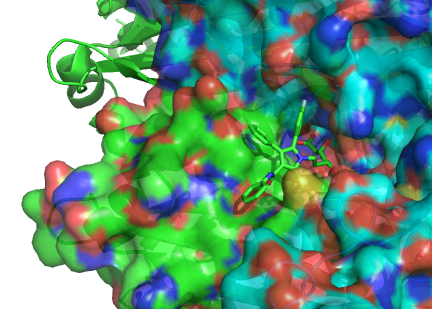
The recently discovered class of statin drugs are now routinely prescribed for people with high cholesterol levels. These molecules lock into one of the enzymes in the liver that helps synthesise cholesterol, thus blocking its production (figure 13). This helps to bring down overall cholesterol levels.
Figure 13 stick model of a statin molecule locked onto the surface of an enzyme.
Cholesterol itself is a fatty substance that is an essential component of the membranes of every cell in your body. It provides vital fluidity for these ever-flexing structures. However, high levels of cholesterol in the blood are known to be associated with plaque formation which narrows the arteries. The fatty cholesterol molecules don’t mix with the watery environment of blood so are carried around the bloodstream in tiny containers called lipoproteins. These lipoproteins come in two varieties: one, called LDL (Low Density Lipoprotein) increases the presence of cholesterol, the other, HDL, reduces it. That’s why we look for low levels of LDL and high levels of HDL in our blood test results.
Cholesterol is brought into our bodies through fatty foods but is also made in our bodies, in the liver. For this reason, levels of it can be reduced in two distinct ways: by reducing the amount of fat in your diet and by taking statins to reduce the internal production of cholesterol.
Blocking a crucial enzyme is also the mechanism used in another important class of heart drugs: beta blockers. These block the action of receptor molecules in heart muscle that respond to adrenalin molecules. Reducing responsiveness to adrenalin has the effect of slowing the heart rate which helps in cases of angina, heart attack, high blood pressure and irregular rhythm.
These kinds of drug treatment are one important way in which the risk of heart disease can be reduced; physical interventions are another. Helen, in one discussion group explained how one of these had helped her brother when he was 13 years old. His aorta was dangerously narrow and had to be expanded. He was treated by a procedure known as “balloon angioplasty”.
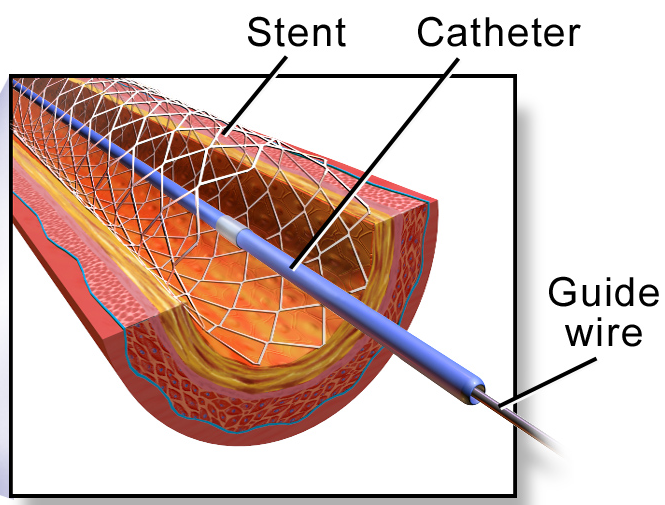
A thin hollow tube with a deflated balloon at the tip is inserted into an artery in the groin. From there it is pushed through blood vessels until it reaches the narrowed part. There the balloon is inflated to push out the walls to expand the artery. A small, expandable metal tube called a stent may be left there to maintain the widening. A similar process is often used to expand a constricted artery in the heart muscle or elsewhere. This ten second video shows how.
Figure 14 Stent inserted by balloon angioplasty
Helen’s mum had also had a heart condition. She underwent triple-bypass surgery. This involves replacing constricted arteries (three in this case) that supply the muscles of the heart with veins taken from other parts of her body.

Another kind of problem arises if the valves in our blood vessels become defective. These are natural pieces of tissue that open and close in a way that ensures our blood flows in one direction only. Artificially engineered alternatives have been developed to replace these; they work effectively for many decades. One particular type is shown in figure 15.
Figure 15 artificial heart valve
Problems with electrical disorders can also be treated with beautifully engineered products. High profile cardiac arrests have made us all aware of the importance of defibrillators, now installed widely in towns and villages across the UK.
By placing the two paddles on the chest one on each side of the heart and applying hundreds, or even thousands, of volts between the paddles for a short time, a large current is passed through the heart muscle.
The process is not fully understood but, in successful cases, the chaotic activity of the heart’s internal pacemaker is, in effect, reset and normal rhythm returns.
Figure 16 defibrillator in action

A small defibrillator (ICD) implanted in the chest of a patient is capable of detecting faulty rhythm (arrhythmia) and delivering a shock immediately if one is detected. This device differs from a pacemaker, which is used to regulate a heart that is beating too slowly. It monitors the heart rate and, if necessary, sends electrical signals to the heart to correct the pace.
Conclusion
With increasing levels of disease associated with the heart, lungs and arteries, we are more aware than ever of the potential risks and the remedies available. This blog has deliberately avoided offering advice on specific conditions or treatments. This is because the detail is important and specific to individual cases. What it has tried to do is provide background information about how the system works so that, if and when heart disease does affect you or those you know, you have a better chance of interpreting what the professionals are telling you. It also offers the purely educational benefit of helping you understand more about another intricate and beautiful aspect of the natural world.
© Andrew Morris
