
“It’s my blood pressure – it always goes up when I run”. “Are you sure – isn’t that’s just your pulse speeding up?”. Such was the confusion arising after Marion had started a discussion about the heart, following her mother’s heart attack. Many other doubts and queries followed, revealing just how central the blood system is to our everyday lives. In this blog we look at how the system works, where it goes wrong and what can be done when it does so.
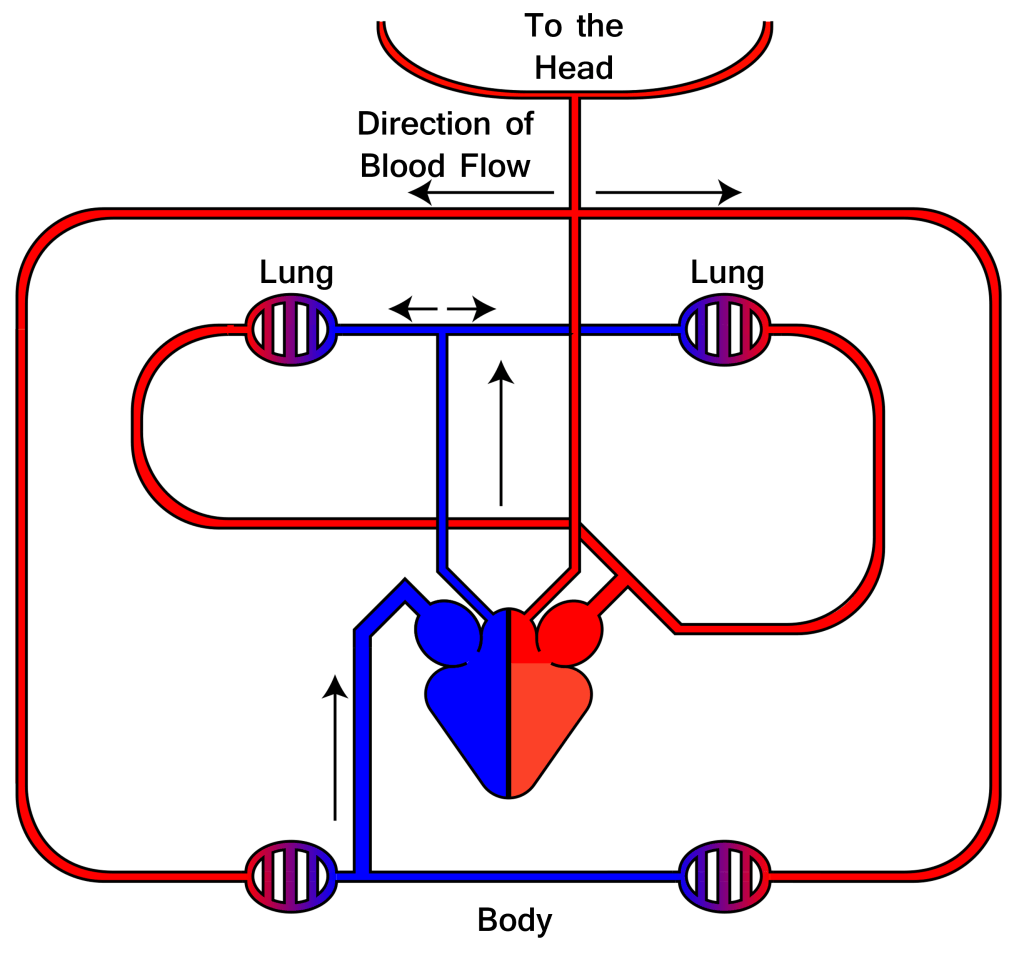
Figure 1 diagram of the blood circulation system
Picking up oxygen
The starting point for the discussion group was the most fundamental question: what is blood for? A quick brainstorm soon came up with many obvious functions: getting oxygen to where it’s needed; transporting nutrients to the muscles; keeping you warm; circulating hormones around ….. it quickly became clear that blood plays many roles, and that circulation is a key feature.
We take the idea of circulation for granted today but before William Harvey’s revolutionary work in 1628, it was believed that blood was simply produced in one place and consumed in another. The prevailing medical authority, the 1st century AD physician Galen, taught that dark blood in the veins comes from the liver and bright blood in the arteries, from the heart. These one-way systems distributed blood to the organs of the body where it was consumed. By conducting carefully designed experiments, Harvey came to the radical conclusion that there was just one single system, in which the same blood flowed round and round, with the heart acting as a pump. In one simple calculation he estimated the amount of blood the heart pumps out every beat and multiplied by the number of heartbeats in a day. This showed it would impossible for the liver to produce enough in a day (over two hundred litres) – it must be continually recycled.
We now know that there is a certain volume of blood moving around the circulation system – approximately five litres on average. The differing colours in the two halves arises because blood changes colour when it takes up oxygen, turning from dark red to ‘bright’ red. This amazing transformation takes place in the lungs. The vital agent that picks up oxygen there and releases it throughout the body is a molecule of a protein known as haemoglobin.
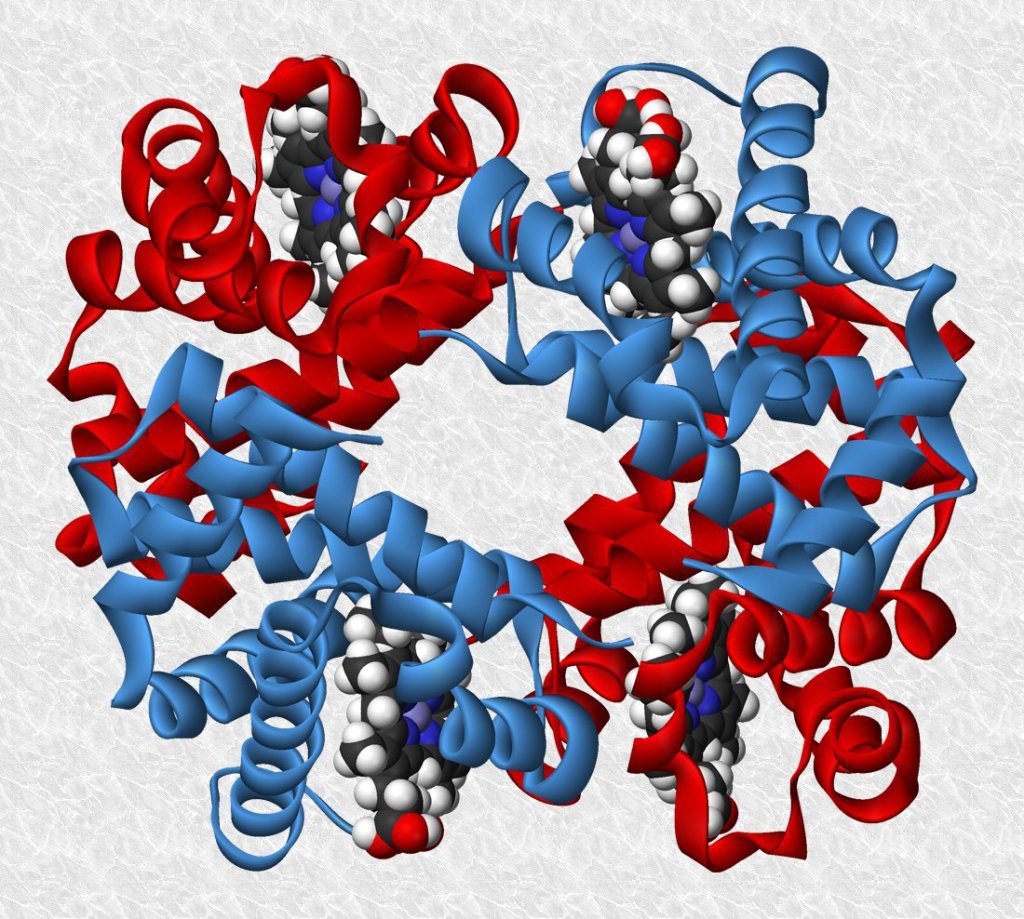
This very large molecule is made of four closely related subunits, depicted in figure 2 as two red and two blue zones. The curly strips, looking like tagliatelle, are representations of the long chains of atoms that make up the giant protein molecule.
Buried in the four quadrants of the molecules are four smaller molecules, known as haems, shown in this diagram as clusters of red, white and dark blue balls, each of which represents an atom. It’s these haem molecules that get hold of oxygen molecules in the lungs and carry them around.
Figure 2 model of a haemoglobin molecule
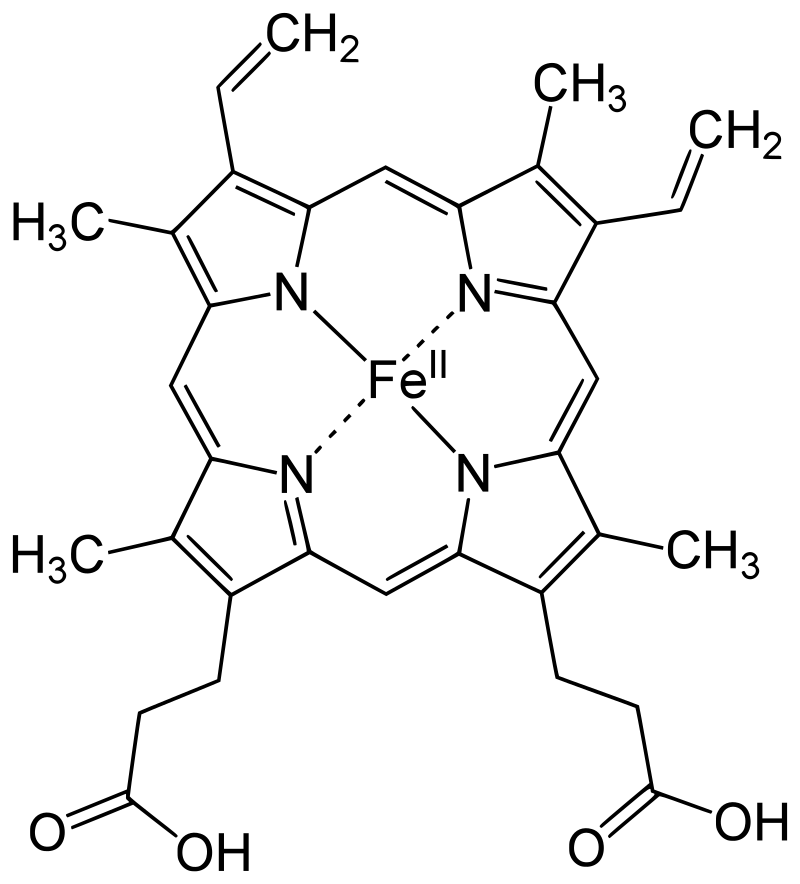
At the heart of each haem molecule is an atom of iron, labelled FeII in Figure 3. It’s the bonding of an oxygen molecule to this iron atom that does the business – just as occurs when oxygen in the air combines with iron when it rusts in damp conditions.
| Figure 3 Haem molecule with an iron atom at the centre |
Deep in the tissue of the lungs are tiny blood vessels, known as arterioles. Oxygen molecules from the air we breathe pass through the ultra-thin lining of the lungs into these tiny vessels. Blood flowing through these arterioles contains a vast number of red blood cells each of which contains hundreds of millions of molecules of the haemoglobin protein. Oxygen molecules from the lungs attach to the iron atoms in the haemoglobin in these red cells.
Establishing the structure of the giant haemoglobin molecule was the towering achievement of Max Perutz, a Jewish refugee scientist from Austria. He dedicated most of his professional life at the University Cambridge to solving this one big problem – which he did in 1959, earning him a Nobel prize.
The animated model in figure 4 shows how the fourfold structure of haemoglobin enables the molecule to pick up oxygen molecules in one environment (the lungs) and release it in another (the tissues).
The binding of an oxygen molecule to the iron atom causes the whole molecule to change shape (labelled Oxy on the right-hand side). When the haemoglobin molecule reaches the distant tissues of the body it gets surrounded by carbon dioxide molecules which switch the haemoglobin molecule to its Deoxy shape, releasing the oxygen it is carrying. What an amazing story of a molecule able to tense up and relax, enabling it to load, transport and unload a cargo!
Figure 4 Haemoglobin molecule, with and without oxygen
Getting around the body
Amy in the group discussion had thought blood was actually blue in the body but only turned red in contact with air. In fact, it simply changes from a darker to a brighter shade of red when it binds to oxygen in the lungs. The reverse happens as it loses oxygen in the tissues. The blue colour used in diagrams is misleading, in this respect.
Oxygen is needed everywhere in the body because every cell depends on it, in order to release energy from the glucose we get from our food. To reach every part of our bodies, the system of blood vessels branches out from the heart, like a tree, into every finer tubes.
| Figure 5 Heart and major veins and arteries |
The network of arteries begins at the heart with the largest of all, the aorta, then branches into multiple arteries which branch in turn into smaller arterioles. Blood returning from the tissues, passes from the smaller venules, into larger veins and ultimately into the two large veins, the venae cavae, to enter the heart (figure 5).
A key question put by Sarah was “where do arteries stop, and veins begin” – or, more specifically: where does the oxygen get dropped off? “Surely, there can’t be a precise boundary like a national frontier?”, she added.
It’s true, diagrams and models like Figure 5 miss out the vital micro vessels where the oxygen is actually deposited, rather than being simply transported. These are the essential unloading places, all over our bodies, where the blood passes though such fine vessels that their very walls are porous to oxygen. These so-called capillaries (figure 6) are too numerous to be depicted in a whole-body diagram.
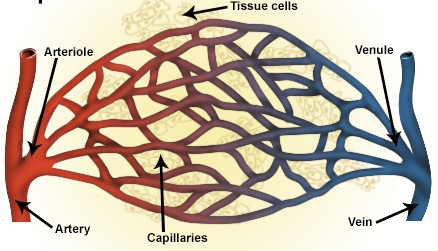
Figure 6 Capillaries
The walls of capillaries are very thin indeed, just one cell thick. This allows many kinds of small molecule, including oxygen and carbon dioxide, to pass through the walls in a way that is impossible through the thicker walls of the larger veins and arteries. In the networks of tiny capillaries throughout the body, oxygen molecules detach from their haemoglobin carriers, pass through the walls and into the various cells that constitute the surrounding tissue. There, they energise the cells in a kind of combustion process, known as cellular respiration. Carbon dioxide, a waste product, passes back out from the cells into the bloodstream. The circulation system described so far takes oxygenated blood from the heart to the various tissues around the body and returns the oxygen-depleted blood back to the heart. But, of course, the blood has to get re-oxygenated in the lungs, ready for the next cycle. For this, a second circulation system is in place The dark blood, lacking oxygen, is pushed back out of the heart into the lungs where again it passes through a network of tiny capillaries (see Figure 1, blue side). The haemoglobin molecules pick up oxygen molecules again and the blood is returned to the heart for re-circulation.
The heart
Any system that moves around fluids – like oil, gas or water – needs a pump to overcome friction at the walls of the tube and viscosity within the fluid. The heart fulfils this role, thanks to strong muscles in its walls that contract regularly.
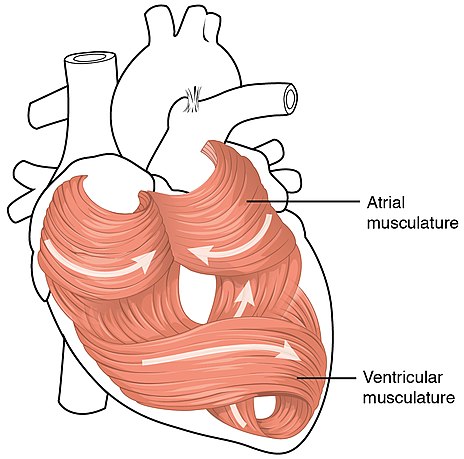
These cardiac muscles are arranged so as to squeeze out the maximum quantity of oxygenated blood from the lower left half (called the left ventricle) to circulate throughout the body. As you can see in figure 7, this is achieved by different layers of the muscle being at right angles to each other – allowing for both upward and sideways contraction plus a twisting movement – like squeezing a wet cloth dry.
| Figure 7 muscles of the heart |
The four chambers of the heart work in a beautifully coordinated way. In the first phase, the upper parts (called atria) are relaxed and suck in both the dark oxygen-depleted blood from the body (on the right-hand side) and also the bright oxygenated blood from the lungs (left-hand side). In Figure 8, we are looking at the front of the heart, so the left-hand side of your heart appears on the right of this diagram.
| Figure 8 the phases of the heart’s cycle |
Subsequently, the lower parts of the heart (called ventricles) squeeze hard to send freshly oxygenated blood around the body (on the left-hand side) and depleted blood into the lungs (on the right-hand side) to pick up oxygen again. This is the systolic phases when the pressure in your arteries is greatest, and you feel a pulse. It gives you the higher of the two numbers when your blood pressure is measured. In between pulses, the situation reverses: the muscles in the upper parts (atria) squeeze blood internally, through to the lower parts (ventricles) to fill them up ready for the next cycle.
It’s almost frightening trying to imagine this coordinated rhythmic movement of the heart. To keep us alive, it simply has to keep repeating its cycle of compression and relaxation all day and night, for a lifetime. We are bound to wonder: what keeps it going, so reliably? What regulates the pulses?
In a sense we know from experience that it must be some kind of electrical system that triggers the muscular rhythm, since a sharp shock from the paddles of a defibrillator can get it going. But, in the special case of the heart, it’s not only nerves that convey the electrical signal but it’s also the muscle itself. Deep in the muscle tissue of the heart, near the top right, lies a spot measuring just a few millimetres, which contains specialised muscle cells that spontaneously charge up and discharge in a never-ending cycle. Charged atoms (called ions) of sodium, potassium and calcium, move in and out of these cells rhythmically. The cycle takes around one second, giving rise to a rising and falling stimulus around 60 -70 times per minute. Thanks to strong connectivity between all the muscle cells of the heart, these impulses spread rapidly across the muscle of the wall. Even more cleverly, they get slightly delayed as they move down from top (atria) to bottom (ventricles). This gives the latter time to fill up fully before they squeeze out their loads.
But, as we all know, our pulse doesn’t always remain steady around 60 – 70 bpm: it can race when we exert ourselves or get frightened. This increases the flow of oxygen to our cells to energise them when extra effort is needed. Clearly the brain must be involved if mental processes, like the perception of a raging bull coming towards us, can raise the pulse rate. A specialised cardiac centre in the brain regulates the heart rate, through a pair of nerve systems. These two are counterbalanced, so that one, driven by the neurotransmitter noradrenalin (or norepinephrine) speeds up the heart rate, while the other, with a different neurotransmitter (acetylcholine), slows down the rate. Under normal conditions, the two are both working in a balanced way to maintain a steady resting heart rate. Under “flight or fight” conditions, however, the brain rapidly sends a signal to the adrenal glands to release noradrenaline, causing the heart rate to speed up. To calm down the heart rate again after an adrenaline rush, a countermanding signal is sent from the brain to the heart via the vagus nerve.
The full picture of heart regulation is a little more complicated, involving a variety of hormones, nerves and receptors. These various systems respond to differing threats, such as shortage of oxygen, excess of carbon dioxide and emotional conditions such as fear. They also do more to deal with a threat than just raise the heart rate – they also widen the arteries to increase the flow of blood where it is most needed, as well as initiating other changes.
Other roles for the blood
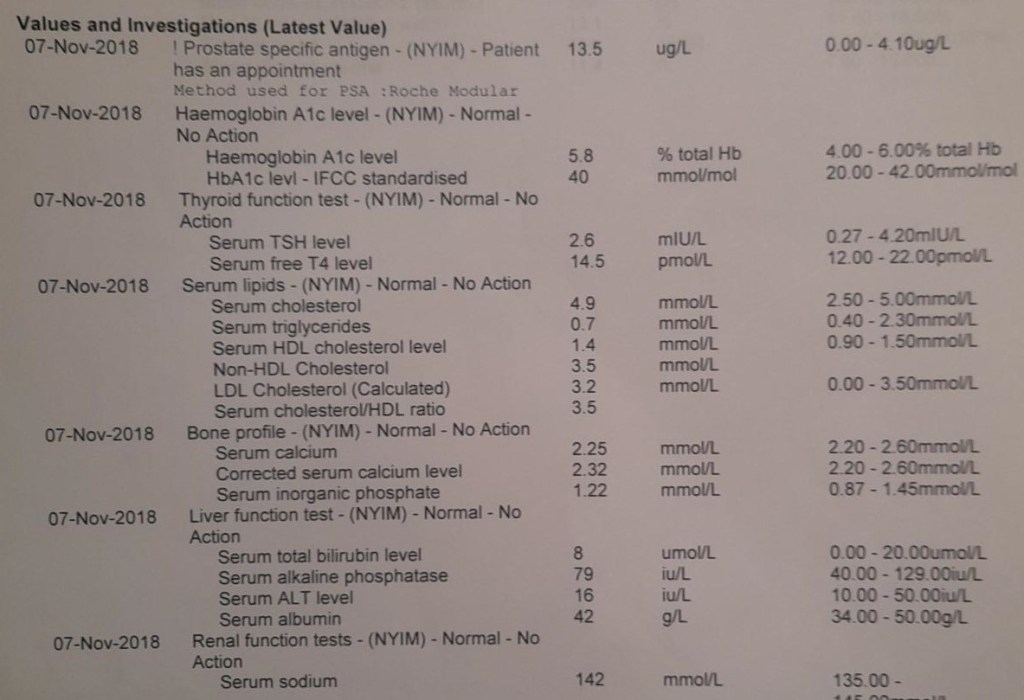
It only takes a routine blood test to remind us how many roles the blood plays, apart from transporting oxygen to the cells. The long and baffling list of results we receive after a blood test offers some clues. A typical example is given in figure 9.
| Figure 9 typical blood test results chart |
The list in Figure 10 gives an indication of some of the other commodities carried around the body in the bloodstream. These include fats and sugars from our intestines; hormones from our glands; carbon dioxide from all our cells; antibodies and white blood cells from the immune system and dead cells and other waste products from the tissues.
If you ever wish to decipher your blood tests results, the chart in figure 10 provides a useful explanation of the abbreviations.
| Abbreviation | Stands for | Description |
| HDL | High Density Lipoprotein | Level of “good cholesterol” in the blood (ratio of HDL:LDL is usually more significant than actual values) |
| LDL | Low Density Lipoprotein | Level of “bad cholesterol” in the blood (ratio of HDL:LDL is usually more significant than actual values) |
| CRP | C-Reactive Protein | Level of inflammation with the body. If the immune system is fighting an infection or illness, CRP will be higher. |
| FBC | Full Blood Count | Analysis of 15 different blood test readings to provide information about overall health. |
| TSH | Thyroid-stimulating hormone | Thyroid regulates the function of metabolism. Low levels can lead to weight loss, while high levels lead to weight gain. |
| PTH | Parathyroid hormone | Regulates serum calcium |
| LFT | Liver Function Test | This test reveals the levels of waste products, enzymes and proteins that are processed by the liver. |
| U+E | Urea and Electrolytes | This test is performed to measure the function of kidney. |
| WBC | White Blood Cell Count | The level of white blood cells. |
| RBC | Red Blood Cell Count | The level of red blood cells. |
| HBC | Haemoglobin | Level of haemoglobin molecules. |
| PLT | Platelets | Platelets levels in the blood. |
Figure 10 meaning of some blood test abbreviations
This partial list is enough to indicate the enormous range of molecules coursing along your bloodstream. Cholesterol is an essential component of cell membranes; C-reactive protein helps rid the body of unwanted material; Thyroid Stimulating Hormone fosters growth and repair; white blood cells help fight infection, red cells carry oxygen around. Taken together, this array of fats, proteins, hormones and cells are reliant on the circulation of the blood to get essential components of the body to where they are needed. As we have seen this may be to muscles, organs like the liver and kidneys and to tissues in general.
The cascading system of blood vessels, from the cavernous aorta, through the branching arteries and narrow arterioles to the tiniest capillaries, ensures these vital ingredients reach every cubic millimetre of the body. Circulating blood is the ultimate transport system. It’s no surprise that the major thoroughfares between our towns and cities came to be known as ‘arterial’ roads.
But, as with road systems, smooth flow can’t always be guaranteed. Traffic levels may rise too high, channels become too narrow, blockages develop, and control systems fail. The heart and blood vessels are prone to each of these threats, causing a variety of cardiovascular ailments. An extraordinary range of innovative treatments have been developed in recent decades to mitigate the effects of some of these, from statins and stents to pacemakers and defibrillators. You can explore some of these in the linked blog 2.19 Ailments of the heart and blood system.
