
“Who’s for coffee?” – a familiar question at the end of a meal. Not so typical was the conversation that followed amongst the family group. One brother declined, claiming it interfered with his sleep; the other chose an espresso and claimed it didn’t affect him.

“Ah – I’ve read about this – caffeine – it’s genetic” chipped in the sister. “How can it be, if they are brothers with the same genes?” queried another. “Hang on; don’t you get some from your mum and some from your dad?” added a friend. “You get a mixture from each, don’t you – one may be blue-eyed the other brown?
It’s not so easy to work out why some siblings look similar and share some of their parents’ traits and other don’t. Even more baffling is how we inherit our parent’s genes yet manage, every one of us, to remain a unique human being. This is the story of inheritance, and the genes that make it happen.
The case of caffeine
Let’s start with the caffeine. It’s true there is a genetic component to our love of coffee … and indeed our individual response to it. According to a review of research somewhere between 36% and 58% of the differences between us when it comes to caffeine can be put down to our genes. Two genes are involved, according to an article in National Geographic; one enables caffeine molecules to be broken down, the other controls the extent to which this happens. As we have become only too aware during the pandemic however, genes can come in various versions: they have variants. In this case, one variant causes caffeine to be broken down rather quickly, so the effects of caffeine will fade more quickly for people with this version. This is just one of the ways we come to differ from one another even if we’re closely related – different versions of the same gene.
Preferences for coffee may seem a rather obscure way to start a discussion on genetics, but what’s true for caffeine goes for all our bodily functions and inherited traits. The same intricate mechanism of inheritance, by means of genes, holds throughout the living world, from the humble yeast to the human brain. We explore here how genes and their molecular partners – the proteins – account for that most universal of interests: how children resemble their parents (or not).
Genes
New born babies are scrutinised by eager relatives for tell-tale features from their mum or dad, or even grandparents. This is entirely reasonable, given that the path of development from the womb onwards is determined largely by the information coded from the very beginning in our genes. Each gene carries the information needed to make one of the twenty thousand odd varieties of protein in our bodies. And proteins go on to shape the way our bodies and minds develop. They make up the tissues – muscle, skin and hair – and act as enzymes, activating vital processes: digestion, breathing, communicating, thinking.
What we become, even as an embryo, let alone as an adult, is determined by the actions of the proteins for which our genes provide the blueprints
We grow tall (or not), for example, largely through the action of a protein called human growth hormone which stimulates our bones to grow. So the particular gene that codes for this hormone influences our height. Somewhere between 60% and 80% of the influence on how tall we grow is genetic according to studies of twins and siblings.
Human Growth Hormone – a molecule of thousands of atoms
Of course, other factors, such as nutrition, play their part in shaping how tall we are – these constitute the other 20% – 40 %.
As with very many aspect of our bodily functioning, it is not only one gene and its corresponding protein that determines the height to which we will grow. Many genes are implicated in the complex process of growth and each of these comes in many versions. Research has uncovered over 700 different variants of the various genes that determine our height.
The complexity of pathways by which genes influence how our bodies work has come as something of a surprise in modern times. There was an earlier expectation that each characteristic of our bodies would be determined by a single gene. This idea has been popularised by the example of eye colour, in which a single gene was thought to provide the code for a single protein which stimulated the production of melanin, the pigment that gives the colour to brown eyes.

Different shades of colour are due to different amounts of melanin and the way it is structured within the eye. The effect of these on the reflection of light from the iris causes a range of colours – much as daylight reflecting off a pigeon’s neck causes colours to appear momentarily.
Image courtesy of LeuschteLampe
To add to the complexity, we now know that no single gene determines eye colour: several different ones play a part, allowing for many possible shades between blue and brown.
The popular idea of a “gay gene” is another example of oversimplified expectations about genes and heritability. As research advances it is becoming increasingly clear that the metabolic processes that shape our physical and mental selves are complex pathways, involving many stages, many proteins and many genes. There’s a long way to go till all of these are understood in any detail, and even further till we understand how they interact with environmental factors.
Nevertheless some characteristics have been found to be determined by a specific mutation in a particular gene and some pathways have been clearly elucidated. Of practical importance is research into the genetic basis of some heritable disorders, including cystic fibrosis, sickle cell anaemia and Huntington’s disease. More about how gene therapy is helping with this is given in the Further Detail section below.
Alternative versions
If some versions of genes are defective, we are bound to wonder why some of us are affected and others unaffected by heritable disorders – or indeed why they survive at all in the population. Why is it that some people carry an unhealthy gene but their children are not affected, whereas those of others are? Is this linked to the taboo on close relatives marrying? Is this why closed communities are keen to widen their gene pool?
As we all know, genes are inherited from our parents. But we have two of these, each with different versions – whose do we get? Sexual reproduction has evolved over the aeons to ensure that we receive two versions of each gene rather than the single version that clones have to manage with. Clearly this offers an advantage if any genes are defective.
This image shows pairs of chromosomes, one from each parent. These carry the genes.
Image courtesy of the US National Human Genome Research Institute
Each parent has, in turn, inherited two versions of each gene from their parents too (hence the possibility of a throwback to the grandparents), and so on back into the mists of time. At the very instant you were conceived the two particular versions of each gene that will stay with you for the rest of your life were determined. Since then almost every cell of your body has descended, by successive divisions, from the original fertilised egg; and each contains identically the same genes.
With two versions of each gene in every cell, we may wonder which one gets used to produce the vital proteins we need – what if it’s a faulty one? It turns out that one version (almost) always dominates over the other – it gets chosen to produce proteins. So provided one of the versions you got from you parents is sound, you will be OK – it will be dominant. However in the unlucky situation that both parents carry a rare, faulty gene, it will be the only choice. This is the cause of the rare genetic disorders mentioned above – sickle cell anaemia and cystic fibrosis for example.
Genetic disorders, as you might expect, capture our attention. You notice if a child has some kind of disorder that one of their parents also has. These are, however, rare and exceptional consequences of an entirely normal process. Genes come in versions (known as alleles) and we always carry two of them in each of our cells, one of them gets chosen as the dominant one when it comes to making the proteins. This is the case for all genes, not just faulty ones.
Genetic roulette
The puzzling thing about family resemblance is that we seem to be like our siblings and parents in some respects and quite different in others. How is it that two acts of conception between the same parents leads to children with utterly distinct characteristics? What is happening to the genes that gives us this endless variety?
The statistical trick is that, with two different versions of each gene available, and over 20,000 distinct genes in a human being, the number of permutations is simply enormous. Imagine a coin tossed 20,000 times and try counting the number of ways it could have fallen. Just toss it twice and you have four ways (HH, HT, TH, TT), toss it three times and you have eight …. imagine 20,000 times; what are the chances of getting 20,000 heads in a row? It’s this kind of unlikeliness that makes us each unique!
So the question of what makes you, you, boils down to which version of each gene gets passed on from your parents at the moment of conception. Amazingly, it’s not so different from coin tossing: there’s only two choices (normally) and random chance determines your ultimate make-up. If any one of a number of random events had worked out differently, a different baby would have been born.
The extraordinary story of gene versions (or alleles) and the way they get mixed in each act of reproduction helps us understand why every individual is unique, yet resembles their close relatives. It’s not the whole story however. Genes go on to instruct the cells in our bodies which proteins to produce. But many other factors will subsequently determine how plentiful and how successful these proteins are in developing us, right through from tiny embryo to ageing adult. Factors in our nutrition, our behaviour, the air we breathe and the stresses to which are subjected will shape our physical and mental development. That would have to be the subject of another whole blog.
To explore the story of DNA, genes and chromosomes in a little more detail, read on.
© Andrew Morris 18th July 2021
Further detail
Genes, chromosomes and DNA
To explore further we need to look at what is going on at the molecular level. A gene is just a short stretch of a long molecule of DNA – the famous double helix. DNA is an extremely long and unwieldy molecule, analogous to a beaded necklace that was 100 kilometers long.

To fit such a long thin threadlike DNA molecule into a microscopic cell it has to be coiled up, like the cable of an old fashioned telephone. And the coils get coiled in turn.
Coiled-up DNA is then compacted, packaged and split up into 23 distinct structures called chromosomes (46 if you count the ones from each parent)
So all the 20,000 odd genes we need for our bodies to function are contained in just 23 distinctive chromosomes and these are replicated in every one of the trillions of cells in our bodies.
It’s the genes in these chromosomes that produce all the proteins that make our bodies work , day in day out, throughout our lives. Genes produce the enzymes that run our metabolism 24/7, the haemoglobin that carries oxygen from our lungs and the proteins that contract our muscles. Genes are in use all the time, throughout our bodies, supplying the code to make our proteins. From time to time however, we need to go beyond merely functioning: we need to go about creating the next generation.
Like the overwhelming majority of animals and plants we don’t do this the simple way: by cloning – making exact photocopies of ourselves. Instead we make new and unique versions of ourselves through the process of sexual reproduction. This ensures that variation is built into the way the species evolves. It enables different versions of individuals to emerge from time to time, by random chance, and a few of these might be better fitted to the environment in which they live. This is how successful species gradually adapt to their ever changing surroundings over very many generations.
So despite its complications in the short term, sexual reproduction beats cloning hands down, in the long run. The complications are less to do with the physical act than with what’s happening at the cellular level. Somehow reproductive cells from two parents, each equipped with two versions of every gene have to mix their four versions together, yet end up with offspring that have only two versions, just as each parent cell has. This is where very special cells come into play – the germ cells that will go on to produce the ovum and sperm. Deep within our glands these special cells are produced in such a way that, unlike all other cells in the body, they end up with only one version of each gene, instead of the usual two. This complicated halving process – called meiosis – takes place in the ovaries and testes.
The germ cells that will go on to produce ova – egg cells – in mature females are already in place in the embryo of baby girls as they develop in their mother’s womb. The ova they will go on to release each month in later years are already present before she is born (though not ready for use yet). The equivalent germ cells that will go on to produce sperm cells in a mature male are also already in place before birth. It Is not until puberty that sperm cells themselves get produced from these forerunners, as a result of hormonal action.
Variation
Variety in our genes is what makes us each a unique individual; it also enables our species (or any other) to evolve over millions of years, as the environment changes. This comes about because the genes we inherit from our mother and father get mixed randomly as our germ cells are created. The chromosomes that carry the genes from our mother and father line up next to each other in such a way that the equivalent genes from each parent lie opposite each other.
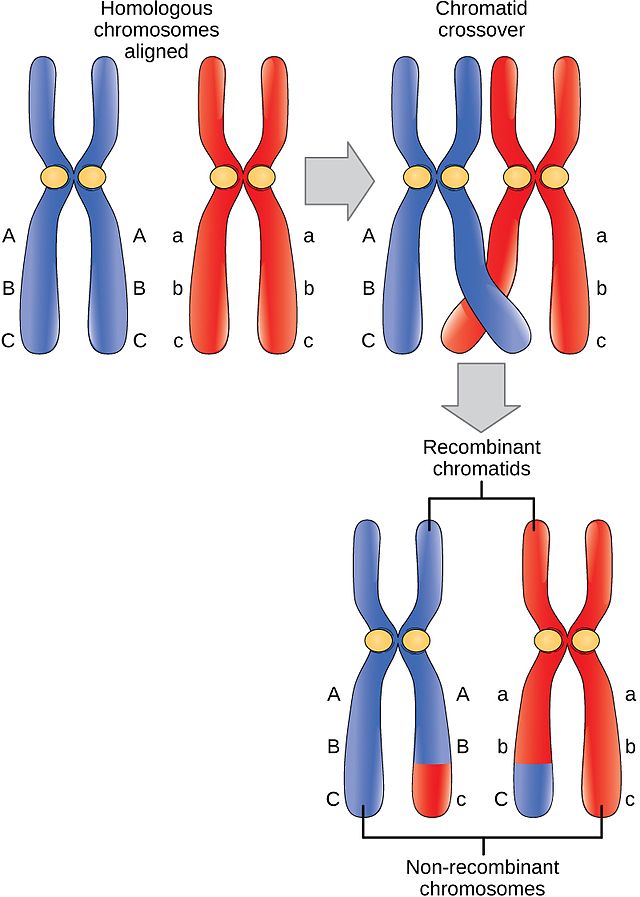
Research in the past 50 years has shown that, when they line up in this way, adjacent DNA molecules – which are carrying the all-important genes – can cross-over or recombine at various points along their length. In this way the version of a gene from one parent (red) can get ‘welded’ into the DNA from the other parent (blue). The result is a novel version of each chromosome, containing a mixture of gene versions from each parent (lower diagram). Amazingly, the mixing is random – there is no way to predict which version will get transferred into which chromosome.
The two newly blended chromosomes then go onto the next stage of reproduction in which just one of them gets chosen to enter the egg or sperm cell. Once again the choice that is made is random.
So there is no way of telling which combination of gene versions (or alleles) will go on to make a new baby.
In fact the unpredictability is even greater than this. Every germ cell that will go on to produce sperm or egg cells is a unique random combination of genes. So every egg and every single sperm cell will be genetically unique. If sperm number one-million-and-two gets there first, it will result in a different baby than if sperm number one-million-and-three makes it first. We are each truly unique, and extraordinarily unlikely, individuals!
But let us not forget that, despite the extreme chanciness introduced by this mixing of gene versions (alleles), all our genes are inherited exclusively from our parents. The pool from which ours are selected is the same as that of our siblings – it’s the particular mix of versions that gets selected that differs. That’s why we are not identical to our siblings but may well resemble them. And what is true for us, was also true for our parents – they inherited their combination of alleles from their parents, and so on throughout our ancestry. This explains how traits from grandparents, or even great grandparents, may appear in later generations – the alleles are passed on unaltered from generation to generation.
Inherited disorders and gene therapy
Some disorders are caused by defective genes that are inherited, usually from both parents.
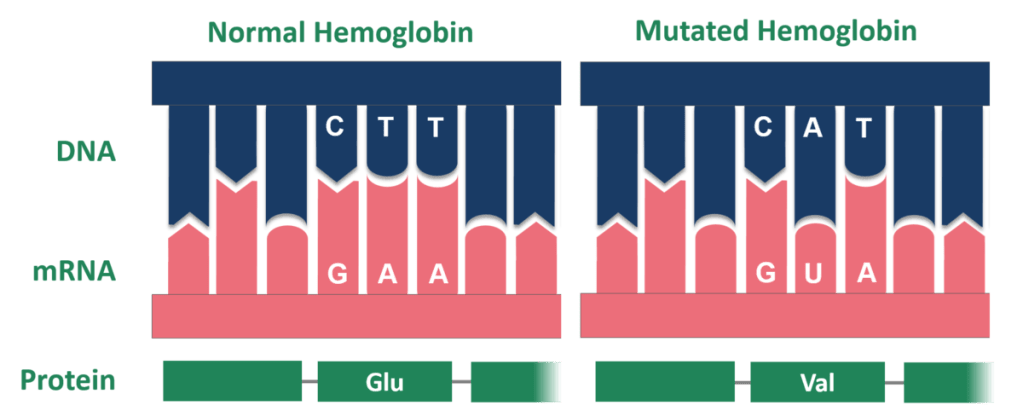
In sickle cell anaemia, for example, one letter in one particular gene that codes for the haemoglobin protein is abnormal. In the diagram, the letter A in the sequence C A T replaces the T in the C T T sequence of normal haemoglobin.
These three letters ensure that a component called Glu (glutamate) goes into the haemoglobin molecule. For people with sickle cell anaemia, however, the CAT sequence means that the wrong component – known as VAL (valine) – is put into the haemoglobin, giving rise to a malformed molecule.
In some cases it has become possible in recent times to correct the fault in the gene through gene therapy. The mutation in a patient’s genes might be corrected or the gene replaced with a healthy one. This promising area of medical research is at an early stage, facing huge technical challenges. Healthy genes have first to be made in the laboratory, then they have to be able to get inside into the relevant cells of the body and finally they have to replace all the old mutated versions.
Amazing progress has been made on each of these in the past few decades, however. In the example of sickle cell anaemia, a beneficent virus is used to break into the cells that make red blood cells in the bone marrow. This exploits the special ability of viruses – getting inside healthy cells – but, of course it’s done in a carefully controlled way. Once inside, these viruses carry the gene for healthy haemoglobin into the cell. Unwittingly the cell starts producing healthy haemoglobin from these imported genes rather than the less effective ones it already had. Red blood cells are refreshed relatively quickly (a matter of weeks) so gradually all the defective cells get replaced. Because of the many technical challenges, however, most genetic conditions have not yet proved amenable to gene therapy. Who knows what research will bring in years to come?
© Andrew Morris 18th July 2021
